ASCVD - Atherosclerotic Cardiovascular Disease

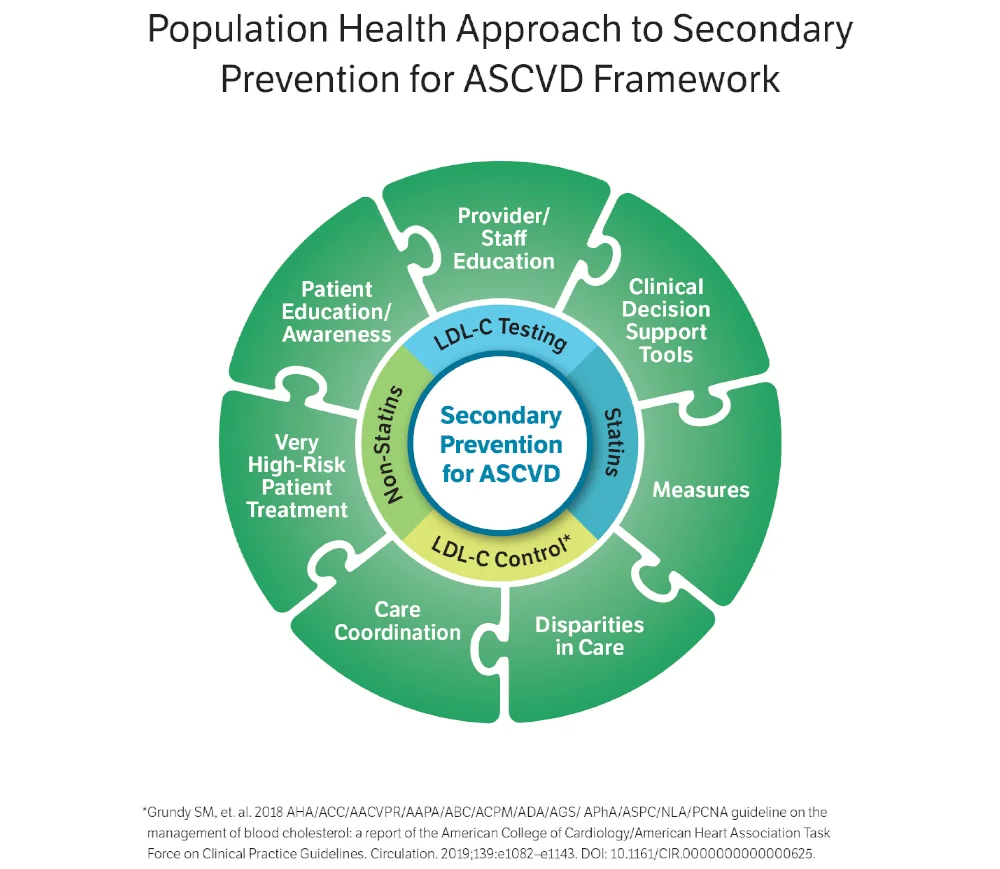
Population Health Approach to Secondary Prevention for ASCVD Framework
Within AMGA Foundation’s ASCVD Best Practices Learning Collaborative, the following motivating needs, as seen in the Population Health Approach to Secondary Prevention for ASCVD Framework, were identified as important or essential aspects to successful patient care in secondary prevention for ASCVD.
Each ASCVD Best Practices Learning Collaborative participating healthcare organization selected motivating needs to focus on for improvement in their organization. Below are interventions developed by the participating organizations.
Participating organizations began intervention implementation in January 2023 and continued until December 2023. During this time, organizations experienced barriers to implementation, such as electronic health record (EHR) changes and delays in queue to make changes in their EHR, health system mergers, staffing changes, etc. Organizations’ work is ongoing, and they anticipate seeing additional improvement in 2024 and beyond, with sustainability efforts.
Motivating Need: Knowledge (Provider/Staff) about patient’s need for secondary prevention for ASCVD
-
Baylor, Scott & White:
-
Host “Lunch and Learns” for providers.
-
Educate the providers that ASCVD patients should have an LDL of <70.
-
Educate and encourage primary care providers about the use of high intensity statins for ASCVD patients or determine why they are not on them.
-
Report data to primary care providers showing the percentage of ASCVD patients that are lacking an LDL.
-
Measurement: Run quarterly reports on ASCVD patients that do not have an LDL and the percentage of ASCVD patients that are lacking a high intensity statin and present data to stakeholders.
-
-
-
Coastal Carolina Health Care: Identified patients not on a statin. Provide standardized education material to patients and encourage use of statins. Identify patients with medication adherence issues and utilize pharmacist as needed. Educated providers on how to overcome statin intolerance and created awareness of the disparity in ASCVD care. Tip: Share transparent provider-level data on a monthly basis. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed high-intensity statin, Baseline 58.0%, Final 58.5%
-
Prevea Health: Create standard education for clinical staff. Create standard patient education materials. Brief provider and staff education.
-
Privia North Texas: Physician education including individualized reporting to increase statin utilization. Create action plan to address low performers. Create patient level reporting by physician of patients that need statin. Create physician specific reports and metrics quarterly. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender Baseline 78.7%, Final 81%
-
PriMED Physicians: Provide documentation of ASCVD risk and patient level goals. Measurement: Organization looked at high intensity statins, LDL goal and any statin usage and compared outcomes for those using Meds Engine vs those who do not.
-
Quincy Medical Group: Educating each provider on their patients who have Coronary Artery Disease who are not currently at goal, and creating an individualized plan for each patient with a care manager. Create a partnership between Cardiology and Primary Care through quarterly meetings.
-
Southwest Medical Associates: Provider Lunch & Learn to educate about statin prescribing, and LDL test ordering. Provider education including one-pager, and Clinical Decision Support Tool. Tip: Continued socialization of ASCVD education tools beyond Primary Care (OBGYN). Measurement: Collaborative measure, Percent of ASCVD cohort prescribed high-intensity statin with LDL measured and controlled at < 70. Baseline 45.8%, Final 47.9%
Prevea Health: “How to talk to patients about the importance of statin” brief provider and staff education
-
Premier Medical Associates: Educate our providers on the importance of utilizing Medisync to ensure best practices in ASCVD care across all populations. Measurement: Quarterly Medisync reports will be run to assess utilization.
-
Southwest Medical Associates: Train providers on use of an enhanced point-of-care EHR tool known as CORE that will identify patients with ASCVD who are not on appropriate statins / and not at goal for LDL cholesterol.
Quincy Medical Group: Acquire list of patients diagnosed with ASCVD. Communicate with all providers via e-mail and provider meetings about the importance of specificity and billing for conditions to ensure their problem lists are up to date and reflect patient conditions.
Motivating Need: Clinical Decision Support Tools
-
Ochsner Clinic: Auto-add ASCVD education to after visit summaries (AVS) at hospital discharge for primary diagnosis with high risk of secondary ASCVD.
-
Premier Medical Associates: An advanced clinical decision support tool was used to guide therapy recommendations for ASCVD patients. After optimizing dose of high intensity statin or adding additional LDL lowering therapies (ezetimibe/PCSK9 inhibitor/siRNA therapy) re-check LDL level within 30 days so additional therapies may be added if needed. Measurement: Collaborative measure, Percent of ASCVD cohort with LDL measured and controlled at < 70, Baseline 27.5%, Final 25.5%*
-
Premier Medical Associates: An advanced clinical decision support tool was used to guide therapy recommendations for ASCVD patients. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed high-intensity statin, Baseline 52.4%, Final 64.4%
-
PriMED Physicians: Developed patient engagement and education tool that helps patient visual results, treatment goal and strength of recommendation. Tip: Make it easy for providers to have conversations with patients by using a tool that is visual for the patient. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender, Baseline 82.9%, Final 86.4%; Collaborative measure, Percent of ASCVD cohort prescribed high-intensity statin, Baseline 49.5%, Final 54.9%
-
Privia North Texas: Address issues such as missing data. Education campaigns. Create EMR workflow and notification process for the end users.
-
Southwest Medical Associates: Implement care guide in EHR to provide standardized evidence based guidelines for management. Use CDS in EHR to identify patients deficient in ASCVD metrics and provide talking points for point of care and metrics for outreach to non-compliant patients.
-
UC San Diego: Revise and initiate health care maintenance alert for LDL Screening. Implement best practice alerts to aid clinical decision making for patients with ASCVD lipid management.
-
Baylor Scott and White: Developed report that generated data for Internal Medicine. Data was shared with the providers to make aware of the “low hanging fruit” that could be tackled. Tip: Provide validated data to get buy in from providers. Measurement: Collaborative Measure, Percent of ASCVD cohort with LDL measured and controlled at < 70
-
Cooper University Health Care: Developed a Health Maintenance care gap notification in the organizations Electronic Health Record System (EHR), allowing providers to receive notifications when a patient with ASCVD, hypercholesterolemia or Diabetes (MIPS #438) is eligible for a Statin Therapy Medication. If a patient has the appropriate diagnoses, providers will receive a notification. The Health Maintenance Gap will be closed once prescribed a Statin or are Statin exclusion is met. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender; Collaborative measure, Percent of ASCVD cohort prescribed high-intensity statin, Baseline 43.9%, Final 45.3%
-
Premier Medical Associates: An advanced clinical decision support tool was used to guide therapy recommendations for ASCVD patients. After optimizing dose of high intensity statin or adding additional LDL lowering therapies (ezetimibe/PCSK9 inhibitor/siRNA therapy) re-check LDL level within 30 days so additional therapies may be added if needed. Measurement: Collaborative measure, Percent of ASCVD cohort with LDL measured and controlled at < 70, Baseline 27.5%, Final 25.6%*
-
Premier Medical Associates: An advanced clinical decision support tool was used to guide therapy recommendations for ASCVD patients. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed high-intensity statin, Baseline 52.4%, Final 64.4%
-
Prevea Health: ASCVD Health Maintenance Topics – LDL and Statin. Creation of Health Maintenance Topic in the EMR to flag patients with ASCVD that are due for an annual LDL measurement and are overdue for statin prescription. Tip: Communicating changes amongst the impacted departments is essential in having staff use these topics for patient care. Measurement: Collaborative measure, Percent of ASCVD cohort with LDL measured and controlled at < 70, Baseline 36.2%, Final 40.5%
-
Premier Medical Associates: An advanced clinical decision support tool was used to guide therapy recommendations for ASCVD patients. After optimizing dose of high intensity statin or adding additional LDL lowering therapies (ezetimibe/PCSK9 inhibitor/siRNA therapy) re-check LDL level within 30 days so additional therapies may be added if needed. Measurement: Collaborative measure, Percent of ASCVD cohort with LDL measured and controlled at < 70, Baseline 27.5%, Final 25.6%*
-
Quincy Medical Group: Utilize Epic to fire a Best Practice Advisory reminding providers that patients with CAD should have an LDL <70; PVD, Carotid Artery Stenosis, and Renal Artery Stenosis should have an LDL <70 and patients with CAD and Diabetes Mellitis have an LDL <100. Educating each provider on their patients who have CAD who are not currently at goal, and creating an individualized plan for each patient with a care manager. Patients with CAD and DM have an LDL <100.
-
Southwest Medical Associates:
-
Collaborate with the Cardiology and Clinical Application Support (CAS) teams to develop and implement Care Guides in the EHR for patients diagnosed with ASCVD in the problem list.
-
Collaborate with the Health Informatics (HI) Team to identify patients not at goal using the defined criteria.
-
Motivating Need: Measures
-
Coastal Carolina Health Care: Identified patients not on a statin. Provide standardized education material to patients and encourage use of statins. Identify patients with medication adherence issues and utilize pharmacist as needed. Educated providers on how to overcome statin intolerance and created awareness of the disparity in ASCVD care. Tip: Share transparent provider-level data on a monthly basis. Baseline 83.1%, Final 83.2%
-
Cooper University Health Care: Developed a Health Maintenance care gap notification in the organizations Electronic Health Record System (EHR), allowing providers to receive notifications when a patient with ASCVD, hypercholesterolemia or Diabetes (MIPS #438) is eligible for a Statin Therapy Medication. If a patient has the appropriate diagnoses, providers will receive a notification. The Health Maintenance Gap will be closed once prescribed a Statin or are Statin exclusion is met. Baseline 70.1%, Final 70.0%
-
Hattiesburg Clinic: Action List Utilization. Identified patients with upcoming appointments to prompt discussions with their physicians addressing ASCVD risk reduction. Also focused on patients in need of high-intensity statin therapy without upcoming appointments to schedule shared decision making discussions with their physicians. In addition to utilizing existing quality care teams to assist physicians in identification of at-risk patients, utilized specialty and primary care clinic manager focus groups to identify care coordination barriers and implement best practices. Baseline 85.2%, Final 86.0%
-
PriMED Physicians: Patient Engagement. Developed patient engagement and education tool that helps patient visual results, treatment goal and strength of recommendation. Tip: Make it easy for providers to have conversations with patients by using a tool that is visual for the patient. Baseline 85.3%, Final 86.4%
-
Privia North Texas: High Risk Patient Identification. Include the ASCVD risk score in the banner on the EMR. This allows physicians the ability to see the risk level of each patient while they are in the clinic. Used the indicator to create list of high risk patient's not on statin report. This allowed for smaller, more manageable lists for clinics to work with. Tip: Keep it easy and keep it small. All clinicians are overwhelmed, so make the changes that don’t lead to additional workload for them or their staff. Baseline 78.7%, Final 81.0%
-
SIMEDHealth: Pre-visit planning for patients with ASCVD and no statin therapy. Encouraging team based approach in coordinating patient’s care (Reporting, Triage, Tasking, Follow Through). Supporting care pathways for referrals to ASCVD specialists, social services, or dietary counseling. Targeting patients without statin therapy or LDL control. EHR message notifications (“tasks”) sent to provider the day before appointment, prompting engagement and intervention at the point of care. Tip: Send accurate and meaningful information. Baseline 77.4%, Final 82.0%
-
Hattiesburg Clinic: Action List Utilization - Identified patients with upcoming appointments to prompt discussions with their physicians addressing ASCVD risk reduction. Focused on patients in need of high-intensity statin therapy without upcoming appointments to schedule shared decision making discussions with their physicians. Utilized specialty and primary care clinic manager focus groups to identify care coordination barriers and implement best practices. Baseline 42.7%, Final 44.6%
-
Premier Medical Associates: An advanced clinical decision support tool was used to guide therapy recommendations for ASCVD patients. Baseline 52.4%, Final 64.4%
-
PriMED Physicians: Patient Engagement - Developed patient engagement and education tool that helps patient visual results, treatment goal and strength of recommendation at visit. Update treatment plan for each subsequent visit until goal is achieved. Tip: Make it easy for providers to have conversations with patients by using a tool that is visual for the patient. Baseline 51.9%, Final 54.9%
-
Baylor, Scott and White: Developed report that generated data for Internal Medicine. Data was shared with the providers to make awareness of the “low hanging fruit” that could be tackled. Tip: Provide validated data to get buy in from providers. LDL control among ASCVD cohort with any statin prescribed.
-
Premier Medical Associates: An advanced clinical decision support tool was used to guide therapy recommendations for ASCVD patients. After optimizing dose of high intensity statin or adding additional LDL lowering therapies (ezetimibe/PCSK9 inhibitor/siRNA therapy) re-check LDL level within 30 days so additional therapies may be added if needed. LDL control among ASCVD cohort with any statin prescribed, Baseline 32.6%, Final 30.7%*
-
Prevea Health: ASCVD Health Maintenance Topics – LDL and Statin. Creation of Health Maintenance Topic in the EMR to flag patients with ASCVD that are due for an annual LDL measurement and statin prescription is overdue. Tip: Communicating changes amongst the impacted departments is essential in having staff use these topics for patient care. Baseline 36.2%, Final 40.5%
-
Quincy Medical Group: Care Manager-Pre-Chart Work-Up. Utilize a Care Manager to preform pre-chart workup the week before on our ASCVD population. Send in-basket message to prescribing provider with most recent LDL, and recommendations for future. Initial focus on Cardiology, have now rolled out to all providers, Cardiology, and Primary Care. Tip: Go all in with all specialties up front. Educate on the recommendations so providers are consistent with their approach. Baseline 29.4%, Final 30.6%
Motivating Need: Disparities in care for patients with clinical ASCVD
-
Coastal Carolina Health Care:
-
Raise awareness among providers and patients about the disparity in ASCVD care.
-
Targeted outreach to patients with ASCVD who have not had LDL in the past 12 months.
-
Schedule pre-visit labs, follow up appointment and enroll patients in care management.
-
Review notes after visit to determine if statin was prescribed. Involve care managers in follow up to review adherence and monitor for side effects.
-
Measurement: Collaborative measures, Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender; Percent of ASCVD cohort prescribed high-intensity statin
-
-
Cooper University Health Care:
-
SDOH assessment of patients with ASCVD.
-
Evaluate patient data to determine age, sex, race disparity in patients without optimized statin therapy and trend.
-
Determine reason for disparity. This could include cost, prescribed/management, and eligibility for use and trend.
-
Create action plan to address disparities.
-
Refer to community/population health to support where needed.
-
Measurement: Collaborative measure, Percent of ASCVD cohort prescribed high-intensity statin, with a focus on female population.
-
-
Hattiesburg Clinic:
-
Action list identifying female patients with upcoming appointments to prompt face-to-face discussions with their physicians addressing ASCVD risk reduction opportunities.
-
Action list of female patients with no LDL in the last year to schedule lab to be completed.
-
Action list of female patients in need of high intensity statin therapy without upcoming appointments to schedule shared decision making discussions with their physicians.
-
Measurement: Collaborative measure, Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender with special emphasis on female population.
-
-
Ochsner Clinic: Increase use of statins in the female population
-
Implementation of PROMPT LIPID
-
Post-event inpatient auto referral to PharmD/lab for education, statin prescribing via written order guidelines with 90-day lab follow-up.
-
-
Premier Medical Associates: Improve prescribing of statins for female patients of PMA with ASCVD. Encouraged providers to use advanced CDS tool to aid management.
-
Privia North Texas: Identify the statin rate by most disadvantaged zip code. Physician education including individualized reporting. Create culturally appropriate patient education.
-
Prevea Health: Rural vs Urban Disparity. Initially started the collaborative with provider education in primary care, implemented updated dashboard metrics and HMT to easily identify patient care gaps and department/provider/organizational level data.
-
PriMED Physicians: Improve prescribing of statins for disparate population (mainly lower income and African American), with use of Meds Engine. Encourage and incentivize providers to use Meds Engine tool as a mechanism to enhance patient engagement. Provide disparate population with care guidelines using patient engagement tools.
-
Quincy Medical Group: Increase Cardiology services provided to the rural population. Meet the patients where they are. Provide education. Increase the use of medication and testing among this population.
-
SIMEDHealth: Women without statins by geographic location (Zip Code). Evaluate difference between high- and low-income areas. Identify women who are at risk, have an upcoming appointment and are not on a statin. Educate providers and clinical staff on proper statin therapy, proper documentation for prescribed as well as reported medications. Measurement: Maintaining elevated statin therapy percentages will allow us to be able to assess the long term patient compliance with statin therapy.
-
Southwest Medical Associates: Improve access & education for female patients. Data review for gaps, non-adherence & appropriate intensity. MA schedule & chart review with provider notification. Patient outreach. Education for clinicians and patients.
-
UC San Diego: Female population focus. Provider education on statin therapies, intolerances, and disparity in the female population. Collaborative outreach with Pop Health pharmacists to reach out to patients on low/moderate statins appropriate for medication titration, prioritizing female patients. Promote referral pathways to (1)Pop Health pharmacists for statin side effects and (2)lipid clinic for increased support for patients with true statin intolerance.
Motivating Need: Care coordination for patients with ASCVD
-
Coastal Carolina Health Care
-
Targeted enrollment of patients with ASCVD in care management. Measurement: Number of patients with ASCVD enrolled in care management
-
Reviewed discharge notification process. Reviewed notification process for discharges and found there is office variation in follow up visits that are scheduled at the PCP’s office vs those scheduled by Cardiology for ASCVD patients. Patients are prioritized according to their readmission risk score completed during the TOC. Measurement: Collaborative Measures, Percent of ASCVD cohort with LDL measured and controlled at < 70, cohort, LDL control among ASCVD cohort with any statin prescribed, LDL control among ASCVD cohort with high-intensity statin prescribed
-
Evaluate and update existing care pathways with Quality Committee. Ensure all clinicians have access to care pathways using shared drive. Communicate to clinicians and staff, request feedback.
-
-
Hattiesburg Clinic:
- Action List Utilization - Identified patients with upcoming appointments to prompt discussions with their physicians addressing ASCVD risk reduction. Also focused on patients in need of high-intensity statin therapy without upcoming appointments to schedule shared decision making discussions with their physicians. In addition to utilizing existing quality care teams to assist physicians in identification of at-risk patients, utilized specialty and primary care clinic manager focus groups to identify care coordination barriers and implement best practices. Measurement: Collaborative Measure, Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender, Baseline 85.2%, Final 86.0%; Collaborative Measure, Percent of ASCVD cohort prescribed high-intensity statin, Baseline 42.7%, Final 44.6%
- Collaborated with their value-based payers to align medication adherence strategies. Embedded pharmacist to improve statin therapy adherence. 90-day prescription refills (required provider and patient education). Assisted enrollment in health plan mail order pharmacy with automated delivery. Case manage patients with a history of poor statin refill adherence.
- Prevea Health: Create standard work documents for care provided for ASCVD patients. Provide follow up with other services including transitional calls, patient education, and medication compliance. Increase offering of prescription for wellness services.
- Quincy Medical Group: Care Manager-Pre-Chart Work-Up - Utilize a Care Manager to perform pre-chart workup the week before on our ASCVD population. Send in-basket message to prescribing provider with most recent LDL, and recommendations. Initially focused on Cardiology, have now rolled out to all providers, Cardiology, and Primary Care. Tip: Go all in with all specialties up front. Educate on the recommendations so providers are consistent with their approach. Measurement: Collaborative measure, Percent of ASCVD cohort with LDL measured and controlled at < 70, Baseline 29.4%, Final 30.6%
- SIMEDHealth: Focus on patients without statin therapy. Coordinate efforts to inform providers of missing statin therapy. Review patient appointments for the next day and send pre-visit planning task to PCP letting them know statin therapy or adjustments to therapy are needed. This includes 90 day prescription adjustments and lab order requests.
- Southwest Medical Associates: Collaborate with the PreVisit team, contact identified deficient patients, with the aim of scheduling an appointment for the patient with the primary care provider team to discuss treatment options.
-
Coastal Carolina Health Care: Model practice identified patients with ASCVD who have not had an LDL in the past 12 months to schedule pre-visit labs, follow-up appointment. Females were identified as disparate patient population. Establish and coordinate dose recommendations and targets between Primary Care and Cardiology. Evaluate and update existing care pathways.
-
Ochsner Clinic: Develop a consistent workflow from both Primary Care and Cardiology regarding post event labs and transition to high intensity statin therapy. Building lab and PCSK9i orders into hospital discharge planning. Develop workflow for enrollment into digital medicine programs. Inclusion of lipids into pharmacy post-hospitalization protocol. Provider education.
-
Prevea Health: Create standard work documents for care provided for ASCVD patients. Provide follow up with other services including transitional calls, patient education, and medication compliance. Increase offering of prescription for wellness services
-
SIMEDHealth:
-
Create a community resources handout/flyer for patients in needed of social services prescription assistance. Utilize FindHelp.org to connect patients to their own local resources. Measurement: Reports built to measure SDOH positive responses and the resources that were handed out. Then cross reference the positive SDOH with the ASCVD patients to identify patients who have ASCVD and SDOH needs to further support those patients through individual outreach.
-
Pre-visit planning for patients with ASCVD and no statin therapy. Encouraging team based approach coordinating patient’s care (Reporting, Triage, Tasking, Follow Through). Supporting care pathways for referrals to ASCVD specialists, social services, or dietary counseling. Targeting patients without Statin therapy or LDL control. EHR message notifications (“tasks”) sent to provider the day before appointment, prompting engagement and intervention at the point of care. Tip: Send accurate and meaningful information. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender, Baseline 77.4%, Final 82.0%
-
-
UC San Diego:
-
Improve Care Pathway by deploying statin prescribing and lipid monitoring health maintenance topics and best practice alerts for primary and secondary prevention of ASCVD to standardize care. Tip: Implement provider education from cardiologist/lipidologist to increase awareness and utilization of pathway. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed high-intensity statin with LDL measured and controlled at < 70, Baseline 39.4%, Final 46.9%
-
Motivating Need: Very high risk patients with clinical ASCVD treatment
-
Coastal Carolina Health Care: Review patients with ASCVD who have medication adherence issues. Identify and assist with potential barriers to taking their medication. Engage care managers and pharmacy consult as needed. Measurement: monitor medication adherence report for patients with ASCVD
-
Cooper University Health Care:
-
Identify patients eligible for statin therapy
-
Increase prescribing high intensity therapy to eligible patients
-
Evaluate provider prescribing practices/knowledge gaps for high intensity statin therapy and provide education session/tools on ASCVD/evidence based prescribing guidelines of high intensity statin therapy
-
Monitor LDL levels
-
Measurement: Collaborative measures, Percent of ASCVD cohort prescribed high-intensity statin; Percent of ASCVD cohort prescribed high-intensity statin with LDL measured and controlled at < 70
-
-
Premier Medical Associates: Cohort of patients who are already on an LDL but are on an incorrect dosage. PharmD’s, Nurses, Quality team members will complete these reach out calls for med dosing changes.
-
Prevea Health: Create standard patient education materials. Coordinate care for patients missing LDL measurement. Standard order set.
Privia North Texas: High Risk Patient Identification. Include the ASCVD risk score in the banner on the EMR. This allows physicians the ability to see the risk level of each patient while they are in the clinic. Used the indicator to create list of high risk patient's not on statin report. This allowed us to give the clinics smaller, more manageable list to work. Tip: Keep it easy and keep it small. All clinicians are overwhelmed, so make the changes that don’t lead to additional workload for them or their staff. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender, Baseline 78.7%, Final 81.0%
Motivating Need: Patient awareness and education about secondary ASCVD
-
Coastal Carolina Health Care: Identified patients not on a statin. Provide standardized education material to patients and encourage use of statins. Identify patients with medication adherence issues and utilize pharmacist as needed. Educated providers on how to overcome statin intolerance and created awareness of the disparity in ASCVD care. Tip: Share transparent provider-level data on a monthly basis. Measurement: Collaborative measure, Percent of ASCVD cohort prescribed high-intensity statin, Baseline 58%, Final 58.5%
-
Cooper University Health Care:
-
Evaluate health literacy where possible
-
Provide education appropriate to learning needs to patients with ASCVD prescribed high intensity statin therapy, which could include Information about ASCVD, medication prescribed for ASCVD, heart healthy diet, exercise
-
Refer to Population Health for Longitudinal Care Coordination
-
Goals setting with patients
-
Measurement: Audit referral frequency to population health & evaluate frequency patient education provided to patients during office visit through chart audit.
-
-
Hattiesburg Clinic: Implement standardized provider education through physician face-to-face peer discussions and sharing of collaborative data to raise awareness and prompt provider/patient shared decision making discussions.
-
PriMED Physicians: Show the patient the screen/print version of their 2nd risks and treatment recommendations together with “Medical Evidence”. Physicians discuss rationale for treatment and show AHA/ACC “evidence”.
-
Quincy Medical Group: Develop consistent and standardized education to provide to patients in Cardiology, Cardiac Rehab, and Primary Offices. Allows patients to understand the importance of a lipid panel, and what their results mean. Medication education, resources for affordability of medications. Small quarterly portal pushes to patients within the cardiac registry with important preventive tips for dietary and lifestyle risks. Marketing team, cardiologists and Primary care providers collaboration to create phrase in EPIC, as well as a handout, that can be given to patients. The portal push will be electronic.
-
SIMEDHealth:
-
Review active statin medications who had less than 30 days issued and monitor for 90 day prescription issued.
-
Create social media campaign to promote the importance of statin therapy with ASCVD (monthly posts). Measurement: review past social media posts for opens, clicks, and website hits.
-
-
Southwest Medical Associates: Providing patients with ASCVD-related brochures and rooming with "Protect Your Heart" Poster: why statins are an important part of good health. Tip: Continued socialization of ASCVD education tools beyond Primary Care (OBGYN). Measurement: Collaborative Measure, Percent of ASCVD cohort prescribed high-intensity statin with LDL measured and controlled at < 70, Baseline 45.8%, Final 47.9%
-
Cooper University Health Care
-
Evaluate health literacy where possible
-
Provide education appropriate to learning needs to patients with ASCVD prescribed high intensity statin therapy, which could including Information about ASCVD, medication prescribed for ASCVD, heart healthy diet, exercise
-
Refer to Population Health for Longitudinal Care Coordination
-
Goals setting with patients
-
Measurement: Audit referral frequency to population health & evaluate frequency patient education provided to patients during office visit through chart audit.
-
-
Premier Medical Associates: Utilize reports, have Quality team and Pharmacy team begin calls to patients. Tasks to providers to add meds, make med changes and/or medication adherence improvement. Portal education on secondary ASCVD education will be sent when appropriate.
- PriMED Physicians: Developed patient engagement and education tool that helps patient visual results, treatment goal and strength of recommendation. Tip: Make it easy for providers to have conversations with patients by using a tool that is visual for the patient. Measurement: Collaborative measures, Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender, Baseline 85.3%, Final 86.4%; Percent of ASCVD cohort prescribed high-intensity statin, Baseline 51.9%, Final 54.9%
For reference:
*Premier had seen increasing rates of LDL control among their patients with ASCVD peaking at 6% absolute improvement in the third intervention quarter. This improvement was consistent with their success moving patients from a low/medium-intensity statin to high-intensity statin therapy (from 59% to 64%), increased prescribing of combination lipid-lowering therapy, and increased LDL testing. In the fourth and final intervention period they saw a marked decline in their LDL control (down 8.5 percentage points in one quarter). Premier documented that this fall was primarily due to ~11% of the ASCVD cohort had LDL control in the prior quarter but now had LDL tests that were outside of the 12-month window required for numerator compliance in the final reporting quarter. They consider this a temporary setback due to the timing of both merging with a larger system and transitioning to EPIC. Efforts are underway to contact these patients and get up-to-date LDL measures. With new systems now up and running, they do not anticipate this happening in the future.
Measures defined throughout
Percent of ASCVD cohort prescribed any statin, stratified by race/ethnicity and gender
Percent of ASCVD cohort prescribed high-intensity statin
Percent of ASCVD cohort with LDL measured and controlled at < 70
Percent of ASCVD cohort prescribed any statin with LDL measured and controlled at < 70
Percent of ASCVD cohort prescribed high-intensity statin with LDL measured and controlled at < 70